Fever (pediatrics)

Fever is a rise in body temperature (core body temperature) above 38 °C.
Body temperature is maintained by a control system in the anterior hypothalamus. Fever is caused by the leaching of endogenous pyrogens into the circulation as a result of infection, an inflammatory process (rheumatic disease) or malignancy. Microbes and their toxins act as exogenous pyrogens and stimulate the release of endogenous pyrogens. Endogenous pyrogens include interleukin-1 (IL-1), interleukin-6 (IL-6), tumour necrosis factor (TNF), and interferons released by monocytes, macrophages, mesangial cells, glia, epithelia and B-lymphocytes. Endogenous pyrogens enter the anterior hypothalamus via the arterial blood circulation, from where arachidonic acid is subsequently released, which is further metabolized to prostaglandin E2, which increases the setting hypothalamic thermostat. Antipyretics (ibuprofen, aspirin) inhibit hypothalamic cyclooxygenase and thereby inhibit the production of prostaglandin E2.

The most common cause of fever is an infectious disease. Life-threatening bacterial infections include, in particular, sepsis, meningitis, osteomyelitis, arthritis, cellulitis (inflammation of subcutaneous fat and ligaments), enteritis, pyelonephritis and epiglottitis.
Thus, fever is caused by the leaching of endogenous pyrogens, the production of which can be induced by exogenous pyrogens (bacteria and their toxins, viruses, yeasts, protozoa, drugs, toxic substances…). However, fever can also occur without the presence of pyrogens, e.g. during intracranial haemorrhage, thrombosis, severe hemolysis, brain tumours, hypothalamic disorders.
Hyperpyrexia
Hyperpyrexia is a body temperature above 40-41 °C axillary. It is usually part of a developing septic shock with manifestations of centralized blood circulation (cold acre, impaired peripheral perfusion, tachycardia). Represents a high degree of risk to the patient (convulsions, disorders of consciousness, risk of dehydration).
Fever phase
- Prodromal (latent) stage (set-point readjustment phase) temperature does not change yet.
- Increment (increase in temperature - feeling cold) the body's effort to prevent heat loss - vasoconstriction, increase basal metabolism (BM), heat generation, muscle tremor (up to 5 weeks of age without tremor - heat production by brown fat), cold, pale skin, cessation of perspiration, thermoregulatory behaviour (reactions similar to exposure to cold).
- Acme (plateau - peak) after reaching the maximum temperature set by the set-point, warm, red, dry skin - increased warm blood flow, increased heart rate (HR) (1 °C 8-10 beats).
- Decrement (retreat - feeling warm, redness) return of set-point and temperature to normal, removal of heat from the body - vasodilation, sweating, warm, red, damp skin, thirst, possible dehydration, pressure drop.
Temperature and its duration depend on many external and internal factors (amount and type of pyrogens, hydration, ambient temperature - heat production increases in the cold, heat loss decrease in the heat = reaching dangerously high values + worsens dehydration, age - the elderly have a lower febrile response, young children are prone to high temperatures, febrile convulsions…).
Metabolic context
- effect on heart rate (1 °C + 8–10 beats / min, risk of heart failure).
- increase in the body's nutritional requirements (energy-intensive condition, increased sympathetic activity, increased metabolic demands, energy savings for the immune system).
- danger dehydration (fluid supply, especially in the elderly), decreases diuresis.
- hyperventilation (increased BM).
- constipation (due to dehydration, decreased intestinal motility).
- hyperreactivity x attenuation of CNS (hallucinations, depression, restless legs syndrome).
- anorexia (TNFα cachectin), protein catabolism (negative N balance), hyperglycemia (increased glycogenolysis, gluconeogenesis).
- febrile convulsions - generalized tonic-clonic convulsions or impaired consciousness when the temperature rises, resolves spontaneously in a matter of minutes, affects children under 5 years of age.
Types of fever

Previously, fever-type was a diagnostic feature. Today, with the use of ATB, corticoids, antipyretics are losing their original meaning.
- Febris continua (continuous) - temperature still above 38 °C, temperature differences during the day are less than 1 °C; e.g. for typhoid.
- Febris recurrens (return) - regular alternation of fever days with fever-free periods; e.g. return typhus.
- Febris remittens (decreasing) - the temperature changes by more than 1 °C during the day, the minimum values do not fall to normal; e.g. rheumatic fever, severe infections.
- Febris intermittens (alternating) - high fever alternates with normal temperature in one day; e.g. sepsis, pyelonephritis.
- Febris undulans (wavy) - the temperature gradually rises, after a few days it reaches a maximum and falls, after a silent period a new wave follows; e.g. brucellosis.
- Febris bifasica (two-phase) - fever has two peaks separated by a period with normal temperature; e.g. viral neurological infections
Fever of unknown origin
Definition
Fever of unknown origin is a temperature above 38 °C and lasts longer than 14 days. The cause is not clear despite careful history, physical examination and routine laboratory screening.
Causes
The most common cause is an unusual course / manifestation of a common disease.
- Systemic infections: cat scratch disease, ehrlichiosis, salmonellosis, mycobacteria, brucellosis, tularemia, leptospirosis, Lyme disease, syphilis, HIV, CMV, hepatitis, EBV.
- Localized bacterial infections: infectious endocarditis, abscess (intra-abdominal, liver abscess, kidney abscess), sinusitis, mastoiditis, osteomyelitis, pneumonia, pyelonephritis.
- Inflammatory diseases: Kawasaki disease, juvenile rheumatoid arthritis, systemic lupus erythematosus, polyarteritis nodosa, rheumatic fever, non-specific intestinal inflammations.
- Malignancies: Hodgkin's and non-Hodgkin's lymphoma, leukaemia, Ewing's sarcoma, neuroblastoma.
- Münchhausen syndrome.
Investigations
- Blood count + differential leukocyte count, CRP, sedimentation.
- liver tests, blood culture, ABB.
- antinuclear antibodies, rheumatoid factor, complement examination (C3, C4, CH 50 ).
- urine examination + cultivation, stool examination.
- throat swab, otoscopy.
- X-ray of the lungs.
- cytology and cerebrospinal fluid cultivation.
- event. HIV, EBV.
Treatment of fever
- hydration (each °C above 37 °C increases physiological fluid demand by 12%)
- antipyretics:
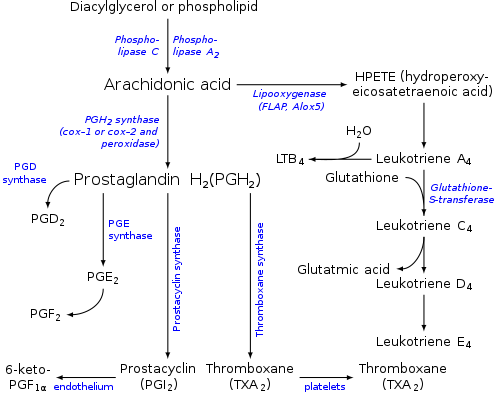
Eicosanoid synthesis - paracetamol
- first-line treatment for newborns.
- dosage: 50 mg / kg / day (in 4 doses); 15 mg / kg every 6 hours, ie 60 mg / kg / day.
- blocks prostaglandin synthesis; metabolized by the liver; maximum effect in 30 minutes.
- side effects are rare (rash, blood disorders).
- the toxic dose is 150-200 mg / kg; clinical signs of overdose: nausea, vomiting within 24 hours after ingestion, pain and tension in the right lower jaw (liver necrosis); liver damage peaks in 3-4 days, followed by encephalopathy, thermoregulation disorder, hypoglycemia, cerebral oedema; plasma level is determined min. 4 h after ingestion.
- antidote: acetylcysteine iv 150 mg / kg in 5% glucose in 15 minutes, then 50 mg / kg in 4 hours, then 100 mg / kg in 6 hours, event. methionine p.o.; hemoperfusion.
- ibuprofen
- for children from 2 months of age, resp. from a weight of 7 kg.
- dosage: 20 mg / kg / day (in 3-4 doses); 5-10 mg / kg every 8 hours, i.e. 15-30 mg / kg / day.
- inhibits cyclooxygenase, i.e. inhibits prostaglandin synthesis; analgesic effect after 30 min. in the length of 4-6 hours, antipyretic effect in 2-4 hours for 4-8 hours; metabolised by the liver and excreted primarily by the kidneys.
- side effects: gastrointestinal bleeding (risk factors: ulcer history, anticoagulant therapy, hepatic impairment), may impair electrolyte secretion in case of decreased renal function.
- clinical signs of overdose: dizziness, nausea, vomiting, blurred vision, hypotension, bleeding, worsening of renal function; there is no antidote.
- treatment in case of overdose: gastric lavage with the administration of activated charcoal, monitoring of vital functions, symptomatic therapy is indicated within 4 hours after overdose.
- acetylsalicylic acid
- up to 15 years - previously the danger of Reye's syndrome.
- dosage: 5–10 mg / kg every 6 hours, i.e. 20–40 mg / kg / day.
- clinical signs of overdose: hyperventilation, tinnitus, deafness, vasodilation, sweating, metabolic acidosis.
- treatment in case of overdose: gastric lavage (even after 24 h), determination of level, control of pO2 and pCO2, replenishment of fluids, forced alkaline diuresis, event. hemodialysis.
- corticosteroids
- hydrocortisone: 30-50 mg / kg / dose.
- methylprednisolone: 1-2 mg / kg / dose.
- metamizole sodium monohydrate (i.m., i.v.)
- dosage: 10-15 mg / kg / day divided into 3-4 doses.
- side effects: risk of agranulocytosis with long-term use; anaphylactic shock.
- paracetamol
- ice infusion

References
Related Articles
- Antipyretics
- Malignant hyperthermia • Hyperthermia • Febrile convulsions • Febrile neutropenia • Sepsis
References
KLIEGMAN, Robert – MARCDANTE, Karen – JENSON, Hal. Nelson Essentials of Pediatrics. 1. edition. China : Elsevier Saunder, 2006. ISBN ISBN 978-0-8089-2325-1.
VAVŘINEC, Otto – VAVŘINEC, Jan. Pediatrie. 1. edition. Praha : Galén, 2002. ISBN ISBN 80-7262-178-5.
KLENER, Pavel. Propedeutika ve vnitřním lékařství. 1. edition. Praha : Galén, 2006. ISBN ISBN 80-246-1254-2.
LEBL, J – JANDA, J – POHUNEK, P. Praktická pediatrie : Obvyklé diagnostické a léčebné postupy na Pediatrické klinice v Motole. 1. edition. Praha : Galén, 2008. ISBN ISBN 978-80-7262-578-9.
