German measles

Rubella (rubella or German measles) is a viral infectious rash. The causative agent is the rubella virus, which is transmitted mainly by droplets. It enters the body through the nasopharyngeal mucosa and causes a disease with a usually mild course. When a pregnant woman becomes infected, the virus spreads across the placenta to the fetus and causes severe congenital rubella syndrome, characterized mainly by severe visual and hearing impairments and congenital heart defects.
Rubella virus
- member of the genus Rubivirus (in former times Togaviridae), family of Matonaviridae, has a genome of single-stranded RNA of positive polarity which is enclosed by an icosahedral capsid.
Epidemiology
The reported incidence of rubella in the Czech Republic in 2005–2009 is 4–14 cases per year, ie 0.1 patients per 100 000 population per year. [1] The source of the infection is a human, with both clinically manifest and clinically silent rubella, from the end of the incubation period to the 7th day after the onset of the rash.[2] A child with congenital rubella can also be a source of infection – it eliminates the virus for many months to years after birth.[2]
Clinical manifestations
The incubation period of the disease is 15-20 days[2], on average 17 days.[3] The infection is spread by droplet infection or transplacentally. The disease is manifested by a maculopapular non-fusing rash, which begins on the face and spreads throughout the body, less pronounced in the limbs. Enanthema to small petechiae, so-called Forscheimer spots, may be present on the mucosa of the palate. The rash is accompanied by swelling of the subocipital and retroauricular lymph nodes.[3]
-
 Rhubarb rash
Rhubarb rash -
 Maculopapular rash in rubella
Maculopapular rash in rubella


Infections in pregnancy
A maternal infection in the first 4 months of pregnancy causes a miscarriage or developmental defects in the fetus. The risk of fetal harm decreases with the length of pregnancy. The fetus is most at risk for maternal rubella in the first trimester.[2]
Gregg's syndrome (congenital rubella syndrome)
Congenitally acquired rubella is manifested by the emergence of the so-called Gregg syndrome:
- deafness;
- congenital heart defects;
- eye disease (typically cataract);
- often also CNS disorders;
- tooth anomalies;
- on the skin purpura or petechia as a consequence of thrombocytopenia;
- sometimes present with hepatitis-induced jaundice.[4]
- late consequences can include autoimmune diabetes mellitus, polyglandular syndrome or rare progressive rubella panencephalitis (PRP).[2]
If a pregnant woman is exposed to an infection in the first trimester and does not have protective antibodies, it is recommended to repeat the serological test in 2–3 weeks and to recommend genetic consultation when antibodies develop.[4] The risk of fetal harm is significant in this situation also offer abortion.
-
 Congenital rubella: skin lesions of the blueberry muffin character
Congenital rubella: skin lesions of the blueberry muffin character -
 Congenital rubella: cataract
Congenital rubella: cataract

_PHIL_4284_lores.jpg)
Complication
Possible complications of rubella include: arthritis, which affects the small joints more often in women[2], encephalitis, thrombocytopenia, and myocarditis.[2]
Diagnostics
- clinical (rash, lymphadenopathy, epidemiological history);[2]
- serology; ELISA
- direct detection of the virus in blood, urine and nasopharyngeal secretion.[2][4]
| CRITERION | Measles | Rubella |
|---|---|---|
| Incubation time | ⌀ 10 days | ⌀ 18 days[2] |
| Temperature | febrile | subfebrile |
| Exanthema | raised, merging, deep red | flat, non-blending, pink (up to mauve) |
| Sowing | behind the ears → nape → torso and limbs | face → torso and limbs |
| Swelling of the nodes | submandibular | nuchal |
| A typical symptom | Koplik's spots (gray macules; buccal mucosa in the stool area) | Forscheimer stains (enanthema/petechiae on the palate) |
| Fetal damage | no | yes |
Therapy
Treatment is only symptomatic, ie based on alleviation. There is no causal treatment. Importantly, patients need to be isolated from a susceptible population.[2]
Vaccination
As part of regular vaccination, the MMR vaccine is given, which contains attenuated measles, mumps, and rubella viruses (measles, mumps, rubella). The first dose is given after the child is fifteen months old. Revaccination is carried out 6 to 10 months after the basic vaccination.[2][5]
Historic window
Congenital rubella syndrome was first described by Australian ophthalmologist Sir Norman McAlister Gregg in the early 1940s, when he linked the increased incidence of congenital cataracts to mothers who have had rubella during pregnancy. Rubella virus was isolated in the early 1960s. This discovery enabled the development of laboratory diagnostics of rubella. In the years 1963–1965, there was an epidemic of rubella in Europe and subsequently in the USA, accompanied by a high incidence of congenital rubella syndrome. These devastating consequences of the rubella epidemic were the motivation for the development of the vaccine. Already in the late 1960s, a rubella vaccine (live, attenuated) was developed and registered, which subsequently became part of the MMR vaccine. Rubella vaccination was started in the United States in young children, while in the United Kingdom in adolescent girls. Neither strategy has led to a sufficient reduction in the virus's circulation in the population, so both countries have resorted to general vaccination of children and targeted vaccination of adolescent girls and adult women.[6]
-
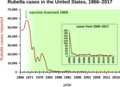 Development of the incidence of rubella in the USA and the effect of vaccination.
Development of the incidence of rubella in the USA and the effect of vaccination.

Links
External links
- DermNet - Rubella
- Pediatrics for practice: Viral rashes of childhood
- Pediatrics for practice: Infectious exanthematous diseases in childhood
Source
- BENEŠ, Jiří, et al. Infekční lékařství. 1. edition. Galén, 2009. 651 pp. ISBN 978-80-7262-644-1.
- ROZSYPAL, Hanuš. Základy infekčního lékařství. - edition. Charles University in Prague, Karolinum Press, 2015. 572 pp. ISBN 8024629321.
Reference
- ↑ STÁTNÍ ZDRAVOTNÍ ÚSTAV,. Vybrané infekční nemoci v ČR v letech 2000-2009 [online]. ©2010. [cit. 2010-08-15]. <http://www.szu.cz/publikace/data/vybrane-infekcni-nemoci-v-cr-v-letech-1998-2007-absolutne>.
- ↑ a b c d e f g h i j k l BENEŠ, Jiří, et al. Infekční lékařství. 1. edition. Galén, 2009. 651 pp. ISBN 978-80-7262-644-1.
- ↑ a b LISSAUER, Tom – CLAYDEN, Graham. Illustrated Textbook of Paediatrics. 3. edition. Elsevier, 2007. ISBN 978-07234-3398-9.
- ↑ a b c KELBLEROVÁ, Aneta. Pediatrie pro praxi [online]. ©2009. [cit. 2021-08-15]. <https://www.pediatriepropraxi.cz/>.
- ↑ MAREK, Petráš. Vakcíny.net [online]. ©2009. [cit. 20. 7. 2009]. <http://www.vakciny.net/pravidelne_ockovani/MMR.htm>. .
- ↑ PLOTKIN, Stanley A.. The History of Rubella and Rubella Vaccination Leading to Elimination. Clinical Infectious Diseases. 2006, y. Supplement_3, p. S164-S168, ISSN 1537-6591. DOI: 10.1086/505950.
