Gallbladder cancer

It is a relatively rare malignancy that affects more of the female population, with median incidence of about 73 years.
Etiology
Higher risk with cholelithiasis or calcified gallbladder, clear RF – ulcerative colitis (9-21 times higher risk). Other – primary sclerosing cholangitis, congenital duct anomalies and parasitic infections.
Clinical picture
Early stages are asymptomatic. Advanced stages have symptoms like other (benign) gallbladder diseases - pain in the right lower jaw, nausea, fatty diet intolerance, anorexia, weight loss and jaundice.
Physical finding
The most common sign of cancer is icterus. We can feel resistance in the right lower jaw, hepatomegaly, ascites may also be found. Non-specific symptoms - pain in the lower jaw, weight loss, pruritus, fever.
Diagnosis
Most are diagnosed at an advanced stage, the main detection methods are CT and US. ERCP is good for localizing biliary obstruction. cholangiocarcinoma can be diagnosed earlier than gallbladder cancer, due to obstruction and jaundice.
many cholangiocarcinomas are considered to be metastatic adenocarcinomas with unknown primary localization.
Histopathology
Adenocarcinomomas account for 85 % and squamous cell or mixed cancers for15 %. Rare – adenosquamous ca, leiomyosarcoma or mucoepidermoid ca.
Bile duct tumors account for 90% of adenocarcinomas.
Treatment
in 1–2 % we find cholecystectomy carcinoma (without previous diagnosis).
Surgical treatment
Surgical treatment is the basic treatment method of early stages, of the proximally located tumors, about 15–20 % are resectable, out of distally located up to 70 %. Resectability is assessed by CT or MRI. For the unresectable, it is important to palliatively bypass the obstruction (bypass, stent). Postoperatively, local recurrences are common - in gallbladder cancer up to 85 %, in bile ducts up to 25–40 %.
Radiotherapy
Radiotherapy can have a palliative effect, brachyradiotherapy is sometimes used in bile duct cancer
There is no evidence of efficacy of adjuvant radiotherapy or radiochemotherapy.
Chemotherapy
Chemotherapy is also used palliatively, mainly 5-FU.
Prognosis
- In the early stages, after a cholecystectomy, the 5-year survival rate is 80%,
- in growth, 5-year survival after surgery is 30%, in nodular involvement 15%,
- median survival after palliative care is 6 months.
-
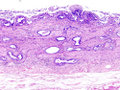 Gallbladder adenocarcinoma, HE staining
Gallbladder adenocarcinoma, HE staining -
 Gallbladder adenocarcinoma, detail of tumor cells
Gallbladder adenocarcinoma, detail of tumor cells -
 Gallbladder adenocarcinoma, lymphatic metastasis
Gallbladder adenocarcinoma, lymphatic metastasis
_histopathology.jpg)
_histopathology.jpg)
_lymphatic_invasion_histopathology.jpg)
Links
Related articles
Source
- BENEŠ, Jiří. Study materials [online]. ©2010. [cit. 16-06-10]. <http://jirben.wz.cz>.
