Skiagraphy
Chest X-ray
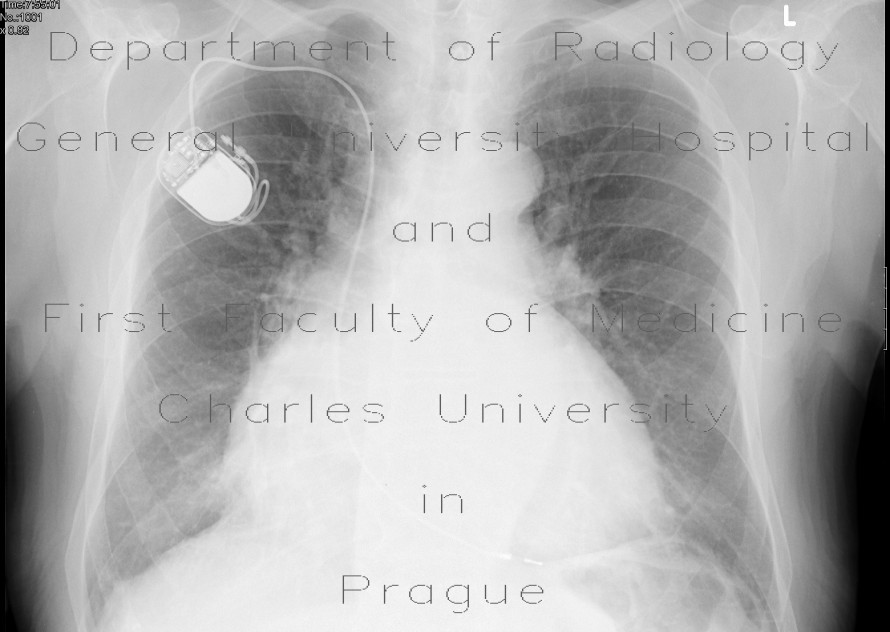
Basic examination method, initial examination for all patients with suspected heart disease. Stand-up RTG of the chest is performed in PA projection (the heart is closer to the detector, there is better sharpness and there is not such a large distortion of the size), ev. with the addition of a side projection. In the picture we see:
- heart shadow configuration: enlargement of the whole heart (heart failure, pericardial effusion), individual compartments, calcification in the cardiac skeleton, tip aneurysmt,
- pulmonary vein filling: congestion, hyperemia,
- pulmonary artery width: pulmonary arch, expansion of the truncus intermedius, "amputation of the hilas" (in pulmonary hypertension),
- aortic arch: elongation or coiled thoracic aorta and atheroma in atherosclerosis, enlargement in aneurysm, reduction in rotation of the heart to the left (in enlargement right ventricle),
- pleural effusion: presence of pleural effusion e.g. in heart failure,
- pulmonary parenchyma: alveolar or interstitial pulmonary edema, Kerley's lines,
- invasion: pacemaker and position of its electrodes, central venous catheter, counterpulsation, Swan-Ganz catheter, artificial valves, sternotomy suture loops, small metal terminals during bypassu.
The so-called "cardiothoracic index", which is the ratio of the widest dimension of the heart (latero-laterally) and the internal width of the chest, is used for an indicative evaluation of the width of the cardiac shadow on the standing PA image of the chest. A cardiothoracic index above 0.5 indicates heart enlargement. This does not apply to the supine image, which is performed in AP projection.
Ultrasound
Echocardiography
The basic functional and morphological examination method of the heart is usually performed by an internist (cardiologist) in most workplaces.
Duplex ultrasound of arteries
It is an ultrasound examination using color flow mapping and spectral curve recording. The examination makes it possible to assess:
- wider lumen: to exclude aneurysmhere or stenosis,
- flow velocity and shape of the spectral curve': flow acceleration at the stenosis site, aliasing (turbulent flow), reduction of pulsatility behind the stenosis,
- course of the artery: anomalous course, duplicated artery, relationship to surrounding organs.
The examination is limited by the depth of the vessel (worse examination of obese patients), calcifications in the vessel wall, patient cooperation and the presence of other interfering structures (e.g. gas in intestinal loops).
Abdominal ultrasound
During an ultrasound of the abdomen, the retroperitoneum is routinely examined (within the limits of visibility given mainly by the patient's habit and flatulence) and the vessels located in it - the aorta and the inferior vena cava. Furthermore, the width of the hepatic veins (widened in right-sided heart failure), the width and the flow of portal vein are evaluated.
Angiography
Digital subtraction angiography enables a better visualization of vascular structures by subtracting the native image (skeleton, soft tissues) from the image when contrast agent is administered. In addition to the imaging of arteries and veins, interventions can also be performed under angiographic control - insertion of stents, dilation, selective embolization.
Selective coronary angiography
Abbreviated SKG, nowadays it is the gold standard in the imaging of the coronary flow and the treatment of coronary arteries. It consists in introducing a catheter Seldinger method (usually from the groin) to the mouth of the coronary arteries. Selective injection of the left and right coronary arteries and their visualization in at least two projections will allow the assessment of the condition of the coronary bed. Part of the stenosis images can then be solved directly by balloon dilation (PTCA - percutaneous transluminal coronary angioplasty) and/or by introducing an expandable stent.
Ventriculography
After the application of the contrast material into the left (less often also the right) ventricle, its kinetics can be evaluated and the ejection fraction, minute cardiac output and systolic volume can be calculated.
Computed Tomography - CT
CT angiography of arteries
CT angiography of the arteries is a CT examination in the arterial phase after the administration of an iodine contrast substance. The examination delay is chosen either according to the usual times, continuous monitoring of the density in the blood vessel (bolus-tracking), or is determined according to the density curve after the application of a small amount of contrast material before the examination (test-bolus). CTA is suitable for examination of the entire aorta and their branches including the splanchnic course, renal arteries and carotid. It reliably excludes aneurysm, dissection, stenosis, bleeding, endoleak, verifies the position and patency of the stent. A limitation of the method is the evaluation of significantly calcified arteries of smaller caliber, where the lumen of the artery cannot be accurately measured due to artifacts from beam hardening.
CT angiography of the pulmonary artery
CTA pulmonary is the method of choice to rule out embolization into the pulmonary canal. In addition, this examination will show or exclude other pathologies in the chest area - mediastinum, pleural cavities and lung parenchyma. At this stage of the examination, the thoracic aorta may not be sufficiently filled, and therefore its possible dissection cannot be ruled out.
CT heart
Most often, CTA heart is performed to assess the state of the coronary artery, further to display the shape of the left atrium before radiofrequency ablation, developmental anomalies and postoperative conditions, for functional examination [ [heart]]. The examination must be performed with EKG synchronization (EKG-gating, EKG-pulsing, EKG-triggering).
Calcium Score
The calcium score evaluates atherosclerotic involvement of the coronary arteries according to the amount of calcified plaques from native CT heart with ECG synchronization. The so-called Agatston score is calculated, which allows for a better stratification of patients according to the risk of coronary artery disease and treatment settings. The calcium score is performed in some workplaces before CTA examination of the coronary arteries - in the case of a high value, CTA is not performed, as it would have limited informative value due to artefacts from calcified plaques. Another importance of performing a native examination of the heart before the CTA of the coronary arteries itself lies in the more accurate determination of the cranio-caudal extent of the examination, the estimation of the risk of movement artifacts, especially of the right coronary artery. Calcium scores cannot be assessed in patients with stents in the coronary artery. The main disadvantage of the calcium score is the radiation load of around 1mSv, which can be reduced by using iterative reconstruction.
CTA of the coronary arteries
Triple rule-out
As the name itself suggests, it is an examination to rule out three pathologies, specifically the most serious causes of acute chest pain − acute coronary syndrome, dissection of the thoracic aorta, pulmonary embolism. The examination is timed so that there is sufficient filling at the same time in the coronary, lung, and thoracic aorta. It is performed acutely in unprepared patients, which reduces the diagnostic yield, especially in the area of the coronary river. Recently, the prevailing opinion is that the clinical and laboratory examination should indicate which of these three pathologies is considered, and the examination should then be aimed at it.
Functional examination of the heart on CT
Classic echocardiography is usually sufficient for a functional examination of the heart. CT and MR allow a more accurate assessment in more complex cases. For CTA of the coronary arteries of patients with a higher heart rate, where it is necessary to capture data throughout the cardiac cycle, a functional examination is a by-product.
CT angiography of veins
CT phlebography
CT angiography of veins is indicated to exclude venous thrombosis in places that cannot be visualized well by ultrasonography, and to evaluate vascular invasion in malignant diseases. The examination is usually performed in the late venous phase (approx. 3 minutes after the application of the contrast agent).
CT portography
This is an examination of the portal watercourse after the application of contrast material in the portal phase. It is used to display thrombosis portal vein, collateral in portal hypertension, TIPSS, infiltration or compression of the portal in expansive processes.
Magnetic resonance - MR
MR angiography
MR angiography of arteries can be performed either natively, using the time-of-flight method and the phase contrast method, or after the application of contrast substance. Compared to CT, there are no calcification artifacts on MR, but MR has a lower spatial resolution.
MR heart
MR heart is most often indicated to rule out myocarditis, cardiomyopathy, to show heart tumors. In myocarditis, we monitor late gadolinium enhancement (LGE) of the affected myocardium. In arrhythmogenic myocarditis, fatty infiltration of the right ventricular wall is usually evident.
Links
External links

 For more information see Heart shadow.
For more information see Heart shadow.
{kind=link}
{kind=link}