Ovarian cysts

Non-cancerous changes in the ovaries (so-called pseudotumors), which are essential for the differential diagnosis of ovarian tumors. They occur either solitary or multiple and can affect one or both ovaries.
They can arise on the basis of changes in the follicles', inclusions of the surface epithelium, or on the basis of endometriosis'.

Cysts on the basis of follicular changes
Follicular cyst
The most common type of cyst. It is probably caused by hyperstimulation of FSH. In essence, it is an "unruptured follicle" that continues to grow and can reach a size of up to 5 cm[1]. The cysts are filled with a yellow liquid with a high estrogen content. They appear in the generation period, either solitary or multiple. They are usually accompanied by amenorrhea. After rupture, delayed menstruation occurs (therefore, when the ovary enlarges, we re-examine the patient after menstruation). If the enlargement persists even after menstruation, we recommend an operative solution. Estrogen production can cause endometrial hyperplasia;
Cyst of the corpus luteum
It arises after the resorption of a larger hematoma, which was formed during the vascularization phase of the corpus. It is smaller and usually bloody. The wall can be up to 3 mm thick, lined by cells containing lutein. Persistent secretion of the corpus luteum cyst results in prolonged bleeding or amenorrhea. May produce progesterone, leading to cycle bleeding disorders. Rupture usually takes place under the picture of abdominal abruption with abdominal bleeding (dif. dg. extrauterine pregnancy) .
Lutein cysts (pregnancy luteomas)
They arise by hyperstimulation of the ovary hCG in trophoblast disorders (mola hydatidosa and choriocarcinoma), but also in normal pregnancy. Cysts can be up to 30 centimeters in diameter and grow very quickly (usually the first sign of trophoblastic disease). They contain a brown liquid, multiple causes enlargement of the ovary. The wall is formed by the ovarian stroma, the lining of the tecolutein cells. After termination of pregnancy or removal of a mole or cancer, they slowly recede (6 or more months).
Polycystic ovary (malocystic ovarian degeneration)
They occur in ``polycystic ovary syndrome (Stein-Leventhal syndrome, PCOS). It affects about 5-10%[2] of women of reproductive age and is a frequent cause of anovulation and infertility. It most likely arises on the basis of a disorder in the synthesis of steroid hormones in the ovaries.
The ovaries are bilaterally enlarged (usually the size of a hen's egg). On the surface, they have a grayish-white tunic albuginea (porcelain ovary) with blue translucent multiple cysts (up to 1 cm). In 70% there is also a higher production of androgens, manifested as hirsutism, also metabolic syndrome, obesity (40%), diabetes mellitus II. type with insulin resistance, cardiovascular disease and an increased risk of developing endometrial carcinoma.
The basis of the treatment is the correction of hyperandrogenemia, adjustment of the cycle and treatment of fertility disorders. During pregnancy, adequate care is needed for the delivery of the fetus, the condition is usually associated with multiple complications during pregnancy. We consider surgical treatment in patients in whom conservative methods do not lead to symptomatic relief. We usually choose point multiple coagulation of cysts with a monopolar needle from a laparoscopic approach[2].
Cysts on the basis of endometriosis
The so-called endometrioid cysts'' (chocolate, Sampson's). In etiology, endometriosis genitalis externa is used. They appear on the ovary, fallopian tube (external), peritoneum in the pelvis, SU ligaments, cervix and form adhesions. The size is varied, from small bearings to (up to 10 cm). They can be a precursor of ovarian endometrial cancer.
Cysts on the basis of inclusion of surface epithelium
Inclusion cysts (Walthard's cysts) are created by ingrowth of the surface epithelium into the ovary. Subsequently, they differentiate into serous, mucinous, salpingeal, endometrial, rare and urothelial. They represent a precursor lesion of ovarian epithelial cystic neoplasms (benign, borderline and malignant).
-
Follicular ovarian cyst
-
 Polycystic ovary syndrome
Polycystic ovary syndrome -
 Cyst in endometriosis
Cyst in endometriosis -
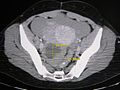 Ovarian cyst on CT
Ovarian cyst on CT -
 Ovarian cyst on ultrasound
Ovarian cyst on ultrasound -
 Hemorrhagic cyst on ultrasound
Hemorrhagic cyst on ultrasound
.png)




Links
Related Articles
Source
- BENEŠ, George. Study Materials [online]. ©2009. [cit. 2010]. <http://jirben.wz.cz>.
- GRUBER, Sarah. Gynecology and Geburtshilfe : BASICS. 5. edition. Munich : Elsevier, 2014. 189 pp. ISBN 978-3-437-42155-6.
- PROMOTED, Ctibor – ŠTEINER, Ivo – DUŠEK, Pavel, et al. Special Pathology. 2. edition. Prague : Galen, 2007. 430 pp. ISBN 978-807262-494-2.
- ROB, Luke – MARTAN, Alois – VENTRUBA, Pavel, et al. Gynecology. 3. edition. Prague : Grada, 2019. 356 pp. ISBN 978-80-7492-426-2.

{kind=link}