Mechanical characteristics of bone joints

The mechanical characteristics of bone joints represent the properties of movements in bone joints. Bones in the body are connected to each other from fixed to highly mobile joints. Bone joints can be divided according to the type of connective tissueinvolved in the construction of the joint. The properties of movement joints (range of motion, flexibility a pevnost) and strength) are not constant during life and change, mainly depending on age.
Connection types by tissue type[edit | edit source]
Fibrous connection[edit | edit source]
The fibrous connection occurs in the form of suture (skull bone), syndesmosis(leg bone at the distal end, but also ligament) and wedging(tooth root and jaw). It is an almost immovable joint formed by ligaments with a predominance of collagen or elastic fibers. It allows only small mutual movements of touching bones.
Cartilaginous junction[edit | edit source]
A cartilaginous joint is a firm but flexible joint using two types of cartilage, hyaline and fibrous. Synchondrosis is a connection by hyaline cartilage, it can be found, for example, in the sternum. The symphysis is connected by fibrocartilage and can be found, for example, at the fusion of the pubic bones.
Bony connection[edit | edit source]
The bony connection is of two types. Synostoses are fixed connections between two bones, created on the basis of ligaments or cartilage. An example is the sacrum, where we find the fusion of vertebrae, that were originally connected by cartilage. If the bones are only in contact with each other and the capsule is on the perimeter of the contact of the bones, we speak of a joint (articulatio). It's a moving connection. An example is the elbow joint or the knee joint.

Knee joint (front view)

Joint[edit | edit source]
Introduction[edit | edit source]
A joint is a movable connection of two or more bones, separated by a gap (joint cavity). The contact surface of the bones is covered by cartilage, the adjacent ends of the bones are covered by a capsule. When analyzing movement, we distinguish between convex joint heads and concaveor flat joint sockets. The type and range of movement in the joint is determined by the size, shape and ratio of the head and socket, the fibrous apparatus of the joint and the muscles located around the joint. The shape of the joint gaps is typical for each joint, their deviations visible on arthrography and CT lead to the diagnosis of the disease.
Structure of the synovial joint[edit | edit source]
Articular cartilage[edit | edit source]
Articular cartilage on the contact surface of the bones is of the hyaline type. It copies the shape of the bones, is flexible and unevenly thick - from 0.5 to 6 mm in the field of its maximum load or in the area where the articulating bones do not significantly match their shape. Cartilage has three layers according to the orientation of the fibers. The upper layer runs parallel to the surface of the cartilage, the middle layer has fibers running crosswise, and the lower layer has fibers embedded in the compacta. Cartilage fibers correspond to its load, most of them go perpendicular to the axis of movement. The deep layer of cartilage is less flexible and forms a transitional layer between bone and cartilage. Cancellous beams the bones in the joint also spatially correspond to the load on the joint - see Mechanical characteristics of bones. This arrangement ensures resistance to pressure and so-called shearing forces.
Cartilage deforms elastically under load. The behavior of cartilage during deformation is determined by the degree of its saturation with synovial fluid. Cartilage is a porous material with holes about 6 nm in size through which synovial fluid. The proteoglycan molecules of the amorphous intercellular mass are able to bind a huge amount of water, under load, the synovial fluid is pushed into the joint cavity and the density of the intercellular mass increases. On the other hand, during relief, the fluid is sucked back by the osmotic forces of the proteoglycans. The flexibility of cartilage is not the same in all joints and also depends on age. In general, the higher the cartilage is, the more flexible it is. Even unloaded cartilage is exposed to a constant pressure of 6–8kg/cm2 due to resting muscle tone. In older people, there is a decrease in chondroitin sulfate and hyaluronic acid and thus a loss of viscosity of the intercellular mass of cartilage - it is no longer able to bind wateras much. It reduces its thickness and the fibrous fibers of the surface layers begin to be exposed, which leads to the disease Osteoarthritis.
Articular cartilage does not have blood and lymph vessels or nerves, nutrition is provided by synovial fluid. If the cartilage is not loaded, e.g. during joint immobilization, it is not nourished and the chondrocytes disintegrate. The metabolism of chondrocytes is very low, because of this the cartilage heals for a long time and poorly, sometimes it cannot heal at all. Nutrition from the vessels of the marginal perichondrium, periosteum and synovial fluid is not enough.
Joint sleeve[edit | edit source]
The articular capsule connects the contact surfaces of the articulating bones around the circumference. Some joints do extreme movement to allow the housing to be quite far from the joints and be loose. Bushings are using mm. articulares stretched to prevent them from being pinched by moving bones. The outer membrane of the capsule is called the fibrous membrane and is mainly made of collagen fibers and ensures the stability and mobility of the joints. In places, it can be strengthened by capsular ligaments, extracapsular ligaments and the beginnings or attachments of muscles. On the other hand, the membrane is weakened in the places of communication with the bursa and in the places where blood vessels and nerves arrive. Ligaments can be made thanks to collagen fibers physiologically lengthen by 4-6% and thus increase the range of motion in the joint. The structure of the fibrous membrane differs in different joints.
The inner surface of the joint is lined with a synovial membrane, which, however, does not attach to the cartilage, articular discs and menisci. It attaches to the bone in close proximity to the cartilage, it can extend slightly to its surface. It is separated from the fibrous membrane by a movable ligament and a number of fat cells. It can extend into eyelashes, villi, fat pads and the cavity separating the septa. The synovial membrane is made up of synovialocytes, flat to cubic cells with microvilli, which enable the transport of substances. However, the layer of synovial cells is not continuous, sometimes the deeper collagen layer also shows through. The cells form hyaluronic acid, which is part of the synovial fluid. We distinguish two types of synovialocytes: type A synovialocytes, phagocytic cells performing a protective function, and type B synovialocytes, which produce collagenous, elastic fibers of the joint capsule and amorphous intercellular mass. Substances consisting of small molecules can be transported through the synovial membrane, which is why we can administer some drugs into the joint cavity.
Synovial fluid[edit | edit source]
Synovial fluid is composed of plasma filtrate, hyaluronic acid and cells (white blood cells or phagocytic cells). The amount of fluid in the joints is not constant, it can be 2–4 ml. Synovial fluid ensures nutrition in the joint, increases and maintains the flexibility of cartilage and reduces surface friction. Hyaluronic acid forms three-dimensional spatial networks that limit the movement of other substances and form a thin layer separating the friction surfaces of the cartilage, which wear out less.
Discs and menisci, rim[edit | edit source]
Discs and menisci are cartilaginous plates inserted between the ends of bones. They are not present in all joints. The discus is a solid plate, dividing the gap into two spaces, the meniscus is sickle-shaped, high at the edges and decreasing towards the center. Both structures are made of fibrocartilage. Their function is to equalize unevenly curved joint surfaces, with their movement they increase the range of motion of the joint, they flexibly deform under load and thus absorb part of the energy under load and improve the flow of synovial fluid, so that it does not cause turbulence and thus poor nutrition of the joint.
The labrum articulare or, cartilaginous rim increases the area of the socket of the bone joint and thus increases the stability of the joint. The hem can be found, for example, at the shoulder or hip joint, where the head is disproportionately larger than the socket and dislocations would easily occur.
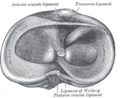
Menisci (top view)

Movements in the joint[edit | edit source]
A negative pressure is stably maintained in the joint gap so that the joint surfaces touch. Movements in the joints can be divided into angular and translational movements. Angular motion is a motion in which all points of the moving object describe circular arcs centered on the axis of rotation. It is typical for the joints of the limbs. A translational movement is a movement in which the points of the moving body describe the same path, it could be compared to sliding, typical of flat joints. Joint kinematics usually involve a combination of both of these movements. Movements can be related to a system of three mutually perpendicular axes – frontal X axis, horizontal Y axis, median Z axis. Thus, abduction and adduction, occur around the X-axis, around the Y axis of flexion and extension and around the Z axis of internal and external rotation. However, no joint is geometrically ideal in its shape, nor is its movement. Any physical activity usually puts a strain on several joints at the same time. There is also a very close relationship between the function of muscles and joints, the joint itself is passive, the muscles are active. However, if there is a functional disorder of the joint, there will also be a response in the muscles.
Types of joints by connection[edit | edit source]
- Simple joints
- Only two bones meet in a joint - e.g. a phalanx joint.
- Composite joints
- In a joint, more than two bones meet (elbow joint) or the joint contains discs and menisci (knee joint).
Types of joints by shape[edit | edit source]
- Ball joint
- The head and socket form the surface of the sphere, movement is possible according to three mutually perpendicular axes – flexion, extension, abduction, adduction, rotation and circumduction. An example is the shoulder joint.
- Elliptical joint
- The head and socket form a structure similar to a rotational ellipsoid, movement is possible along two axes - flexion, extension, bowing, lateroflexion. An example is the union of the occipital bone and the atlas.
- Saddle joint
- The dimple resembles a horse's saddle and the pommel corresponds to the rider's position. Movement is possible according to two mutually perpendicular axes - flexion, extension, abduction, adduction and rotation. An example of the carpometacarpal joint.
- Cylindrical joint
- The cylindrical joint is of two types. Either it has joint surfaces that are part of the surface of the cylinder and the movement occurs along an axis that is perpendicular to the axis of the bone - extension and flexionare possible . This is found in the phalanx joint. The second variant is a wheel joint, the head of which is part of a cylinder and the movement goes along the axis of the bone - rotation. is possible . An example is the union of the Ulna and Radius.
- Pulley joint
- The hole has a leading edge that extends into the groove of the joint head. Movement is therefore only possible along one axis - flexion and extension, the articulating bones cannot move to the sides. An example is the humero-ulnar joint.
- Flat joint
- Stiff joint
- These are joints with considerably limited mobility. The contact surfaces are uneven or the shape of the cartilage blocks movement. This can be found, for example, in the sacroiliac joint.
Proper examination of the joint[edit | edit source]
The movement pattern of each joint is important - its physiological direction and range of motion. Limitation of movement can be either intra-articular or extra-articular. In addition to movements, the joint can also move, we are talking about joint clearance. The movements are dependent and determined by the shape of the joint surfaces. We cannot perform this movement by ourselves, but it is the basis for all other movements. If clearance is reduced in any direction, momentum is limited. Each joint has its middle or neutral position, in which the ligaments and capsule are maximally relaxed, the tension of the muscle groups is in balance. We fix the joint in this position if damage is suspected. If we want to measure the range of individual joints, we use goniometric methods. The standard method is the SFTR method (saggital/frontal/transversal/rotation).
References[edit | edit source]
- NAVRÁTIL, Leoš – ROSINA, Jozef, et al. Medicínská biofyzika. 1 (dotisk 2013) edition. Praha : Grada Publishing, 2005. 524 pp. ISBN 978-80-247-1152-2.
- ČIHÁK, Radomír – GRIM, Miloš. Anatomie 1. 3. edition. Praha : Grada, 2011. 534 pp. ISBN 978-80-247-3817-8.
- DOKLÁDAL, Milan – PÁČ, Libor. Anatomie člověka : [Díl] 1, Pohybový systém. 1. edition. Brno : Masarykova univerzita, 1991. ISBN 80-210-0292-1.
- GRIM, Miloš – DRUGA, Rastislav. Základy anatomie : Obecná anatomie a pohybový systém. 1. edition. Praha : Galén, 2001. 159 pp. ISBN 80-7262-111-4.