Hypertrophic cardiomyopathy/diagnosis

ECG
The ECG examination is abnormal in approximately 90 % of patients with hypertrophic cardiomyopathy.[1] ECG abnormalities may precede myocardial hypertrophy in carriers of the genetic mutation.[2] The examination has no diagnostically specific features. Voltage criteria of left ventricular hypertrophy, even deep T wave inversion (and other ST-T segment changes) and Q wave are often present. Various supraventricular and ventricular arrhythmias, can be detected , even with the use of Holter monitoring, which is important in the stratification of patients at risk sudden death .[1] [3] [4]
ECHO and magnetic resonance of the heart
Used to assess both hypertrophy of the myocardium, which is very often localized in the area of the interventricular septum, and changes in the valvular apparatus of the mitral valve (including the papillary muscles). In connection with the mitral valve, or even by obstruction of the outflow tract of the left ventricle, the systolic forward movement of the anterior leaflet of the mitral valve (abbreviated as SAM) is described. Mitral valve regurgitation is also documented. From other parameters, the presence of other structural changes of the heart, apical Aneurysm of the left ventricle, the severity of diastolic dysfunction of the left ventricle as well as the presence of obstruction of the outflow tract of the left ventricle using continuous Doppler are evaluated at rest and during provocative maneuvers.[1][3][4]
In this case, the use of magnetic resonance imaging of the heart is important in a more detailed and accurate assessment of the morphology of the heart, ncluding imaging of the apical segments and possible hypertrophy or aneurysm in this location (during echocardiographic examination, this area may not always be clearly visible).[4] It is also indicated for the non-invasive assessment of tissue characteristics of the myocardium by monitoring late gadolinium enhancement (LGE).[4][5] Its presence is indicative of interstitial fibrosis. Usually, LGE is located midmyocardially and has a "speckled character". in Fabry's disease LGE typically occurs midmyocardial basally posterolaterally.[6] Despite certain limitations of technical aspects, the detection of LGE in hypertrophic cardiomyopathy is associated with a higher risk of further progression of the disease and the risk of sudden death.[4] Myocardial perfusion disorders can be detected by a PET scan.
- ECHO a MRI záznamy hypertrofické kardiomyopatie
-
 ECHO image of a patient with Fabry disease and hypertrophy of the interventricular septum and posterior wall of the left ventricle, parasternal long-axis projection
ECHO image of a patient with Fabry disease and hypertrophy of the interventricular septum and posterior wall of the left ventricle, parasternal long-axis projection -
 ECHO image of a patient with Fabry disease and concentric hypertrophy, marked hypertrophy of the interventricular septum with transition to the anteroseptum, parasternal short-axis projection
ECHO image of a patient with Fabry disease and concentric hypertrophy, marked hypertrophy of the interventricular septum with transition to the anteroseptum, parasternal short-axis projection -
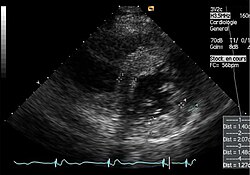
ECHO sequence of the apical form of hypertrophic cardiomyopathy, apical five-chamber projection
-
MRI recording of a patient with hypertrophy of the interventricular septum and an apical aneurysm


Genetic testing and cascade screening
Genetic testing has made significant progress in the field of hypertrophic cardiomyopathy and is particularly important for so-called cascade screening. If a mutation associated with hypertrophic cardiomyopathy is proven in a patient, this diagnosis can be confirmed or refuted by genetic testing in other family members, even those who have not yet developed left ventricular hypertrophy and the general phenotype of hypertrophic cardiomyopathy.[1] However, the situation is complicated by the fact that a specific mutation is identified in only about 50% of patients, and also by the occurrence of mutations in which their association with hypertrophic cardiomyopathy is still unclear (variation of unclear significance).[1] If the mutation is not detected, direct relatives of a patient with hypertrophic cardiomyopathy in the absence of symptoms or other signs of hypertrophic cardiomyopathy are monitored by ECG and echocardiographically in adulthood at most often 5-year intervals. Screening of relatives-children starts already around the age of 12 (sometimes earlier) and here monitoring is carried out at intervals of 12-18 months.[1]
Athletic heart
A certain degree of hypertrophy can be detected even in some elite athletes. Unlike hypertrophic cardiomyopathy, this myocardial hypertrophy is mild (approx. up to 13 mm). If the athlete is in the so-called gray zone (myocardium thickness up to 15 mm), the character of the filling of the left ventricle, the size of the heart compartments, the presence of LGE and sarcomeric mutations are further assessed, when the results of these examinations are not pathological in the case of physiological left ventricular hypertrophy in athletes.[1]
Used literature
- MANN, Douglas L., et al. Braunwald´s Heart Disease : A Textbook of Cardiovascular Medicine. 10. edition. 2015. ISBN 978-0-323-29429-4.
- STANĚK, Vladimír. Kardiologie v praxi. 1. edition. Axonite CZ, 2014. 375 pp. ISBN 9788090489974.
- KUUSISTO, Johanna – SIPOLA, Petri – JÄÄSKELÄINEN, Pertti. Current perspectives in hypertrophic cardiomyopathy with the focus on patients in the Finnish population: a review. Annals of Medicine. 2016, y. 7, vol. 48, p. 496-508, ISSN 0785-3890. DOI: 10.1080/07853890.2016.1187764.
- PALEČEK, T – KUCHYNKA, P. , et al. Nesarkomerické formy hypertrofické kardiomyopatie v dospělosti. Kardiologická revue - interní medicína. 2011, y. 13, vol. 4, p. 210-220, ISSN 2336-2898.
- VESELKA, Josef – ANAVEKAR, Nandan S. – CHARRON, Philippe. Hypertrophic obstructive cardiomyopathy. The Lancet. 2017, vol. 389, p. 1253-1267, ISSN 0140-6736. DOI: 10.1016/s0140-6736(16)31321-6.
- MARIAN, Ali J. – BRAUNWALD, Eugene. Hypertrophic Cardiomyopathy. Circulation Research. 2017, y. 7, vol. 121, p. 749-770, ISSN 0009-7330. DOI: 10.1161/circresaha.117.311059.
- PROF. MUDR. ŠTEJFA, Miloš, et al. Kardiologie. 3. edition. 2007. 776 pp. ISBN 978-80-247-1385-4.
- KAUTZNER, Josef. Srdeční selhání : aktuality pro klinickou praxi. 1. edition. Mladá fronta, 2015. ISBN 9788020435736.
- KUCHYNKA, P. Kardiomyopatie [online]. [cit. 2023-03-27]. <http://int2.lf1.cuni.cz/file/5727/kardiomyopatie-pro-mediky.pdf>.
References
- ↑ a b c d e f g MANN, Douglas L., et al. Braunwald´s Heart Disease : A Textbook of Cardiovascular Medicine. 10. edition. 2015. ISBN 978-0-323-29429-4.
- ↑ KUUSISTO, Johanna – SIPOLA, Petri – JÄÄSKELÄINEN, Pertti. Current perspectives in hypertrophic cardiomyopathy with the focus on patients in the Finnish population: a review. Annals of Medicine. 2016, y. 7, vol. 48, p. 496-508, ISSN 0785-3890. DOI: 10.1080/07853890.2016.1187764.
- ↑ a b STANĚK, Vladimír. Kardiologie v praxi. 1. edition. Axonite CZ, 2014. 375 pp. ISBN 9788090489974.
- ↑ a b c d e VESELKA, Josef – ANAVEKAR, Nandan S – CHARRON, Philippe. Hypertrophic obstructive cardiomyopathy. The Lancet. 2017, y. 10075, vol. 389, p. 1253-1267, ISSN 0140-6736. DOI: 10.1016/s0140-6736(16)31321-6.
- ↑ MARIAN, Ali J. – BRAUNWALD, Eugene. Hypertrophic Cardiomyopathy. Circulation Research. 2017, y. 7, vol. 121, p. 749-770, ISSN 0009-7330. DOI: 10.1161/circresaha.117.311059.
- ↑ PALEČEK, T – KUCHYNKA, P. , et al. Nesarkomerické formy hypertrofické kardiomyopatie v dospělosti. Kardiologická revue - interní medicína. 2011, y. 13, vol. 4, p. 210-220,
