Hyperkalaemia is an increase in the level of potassium in the blood. Normal values are 3.8-5.0 mmol / l. Hyperkalaemia becomes clinically significant when the level rises above 6 mmol / l, dangerous when it rises above 7 mmol / l. As potassium depends on acid-base balance, it should be considered in relation to pH (see Relationships between acid-base balance and ionogram ).
With hyperkalemia, the body's total potassium stores may be increased, normal or decreased!
Causes
Potassium retention
increased income ,
administration of a rapid infusion with K + ,
transfusion of old blood with erythrocyte breakdown,
food only in impaired kidney function,
reduced elimination ,
in the oliguric phase of sudden renal failure (in chronic failure, the disorder is due to a change in the distribution of K + between ICT and ECT),
reduced secretion in tubular disorders (cells are not sensitive to aldosterone ),
in catabolic conditions (in which protein-bound K + is released),
in insulin deficiency (supports the transfer of K + into cells),
when administering β-blockers (they antagonize the action of adrenaline ),
With longer duration of acidosis, potassium depletion develops with concomitant hyperkalemia!
Pseudohyperkalemia
Apparent hyperkalaemia, which may be caused by incorrect blood collection during prolonged venostasis (long strangulation, prolonged exercise) or haemolysis (eg old sample).
Potassium affects the processes on the membrane, so the changes mainly concern exciting tissues. At higher levels of extracellular potassium, the concentration gradient decreases so that potassium escapes from the cell more slowly. This makes the resting membrane potential less negative. In the initial phase of hyperkalemia, irritability increases (resting membrane potential is closer to the threshold). However, as the potassium increases further, the potential for a block of voltage-gated sodium channels increases and the irritancy decreases.
Causes of changes in the origin and conduction of excitement
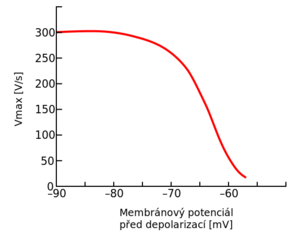
Dependence of the depolarization rate on the value of the resting membrane potential
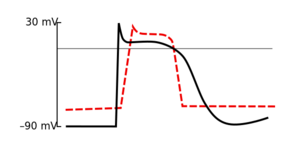
Membrane potential of cardiomyocyte in hyperkalemia
In hyperkalemia, the formation and conduction of excitement on membranes is affected by several mechanism
The potassium concentration gradient in the direction from the intra- to the extracellular space is a key factor determining the value of the resting membrane potential . Increasing the concentration of extracellular potassium leads to a decrease in the gradient, to a decrease in the flow of K + ions from the cell, and thus to a decrease in membrane potential negativity (eg in a cardiomyocyte, the resting membrane potential decreases from −90 mV to −80 mV).
By reducing the negativity of the resting membrane potential, the difference between the resting and threshold potentials is lower and may therefore be easier to induce depolarization. However, as the negativity of the resting membrane potential decreases further, the negativity of the threshold potential also begins to decrease (ie the values no longer approach each other).
The resting membrane potential value determines the number of sodium channels that will be "willing" to activate during depolarization and allow Na + to enter the cell. The less negative the resting membrane potential, the fewer sodium channels are activated and the slower the depolarization .
Repolarization is realized by opening potassium channels and the flow of K + ions from the cell. For unclear reasons, the amount of potassium that flows out of the cell during repolarization increases paradoxically with increasing concentration of potassium in the extracellular fluid. Thus, in hyperkalemia, repolarization is accelerated .
ECG changes then arise as follows:
The earliest manifestations of ECG hyperkalaemia are pointed and narrow T-waves (their shape resembles an Eiffel Tower). Their origin is probably due to the shortening of the action potential and the acceleration of repolarization .
The QRS complex expands and the PQ interval lengthens . These changes are due to slowed depolarization .
With increasing potassium, atrial activity (and P waves) may disappear. The ventricles are then stimulated with an AV node, which is more resistant to these electrolyte changes. So we can register bradycardia.
As the hyperkalemia further deepens, the QRS complex, which may attach to the T-wave, continues to expand, creating a sinusoid-like curve. At this stage, there is a risk of ventricular fibrillation and arrest.
However, changes on the ECG can be diverse - there are tachycardias, bradycardias, changes in the length of PQ and QT intervals, blocks. In some cases, severe hyperkalaemia may even be present without any manifestation on the ECG.
Calcium iv - reduces the risk of malignant arrhythmias (stabilizes cardiomyocyte membranes by an unclear mechanism, among other things shifts the threshold potential to less negative values ): Calcium chloride 10% 25–50 mg / kg (0.1–0.2 ml / kg) 10 ml to an adult , or Calcium gluconicum 10% 0.5–1 ml / kg. The onset of action is immediate, lasting about 30 minutes.
Circulation adjustment
Hypovolemia potentiates and causes all kinds of kidney failure. Diuretics alone in a hypovolaemic oliguric patient can lead to severe kidney damage. Evaluation of patient hydration and volume replenishment is essential.
Potassium transfer into cells
Insulin covered with glucose (insulin increases K + uptake into cells): 1 .mu.l of insulin covers 5 g of glucose. Glucose 0.5 g / kg + insulin 0.1 j / kg within 30 minutes iv Effect noticeable after approx. 30 minutes.
Bicarbonate - especially in case of metabolic acidosis : 50 mmol (children 1-2 mmol / kg) iv, use 4.2% solution. The effect lasts about 30 minutes. Calcium should be given before the administration of bicarbonate - a change in pH leads to a reduction in ionized calcium.
β 2 agonists (increase K + entry into cells): administration of inhalation Ventolin (salbutamol) 4 μg / kg / 20 min in 20 ml FR. Bricanyl (terbutaline) administration: 4-10 μg / kg / 20 min in 20 ml FR. The application of iv is not more advantageous than inhalation in this indication. The effect after about 30 minutes and lasts 2-3 hours.
Removal of potassium from the body
Hemodialysis - a necessary solution for persistent oligoanuria
Furosemide with concomitant saline. Furosemide 0.5-2 mg / kg, but the effect in the acute phase is small and starts with latency. In prerenal renal failure (decreased filtration due to insufficient blood supply), hydration is required, not just furosemide. Loop diuretics do not reduce mortality or renal function adjustment. (Merta 2009) If loop diuretics are administered, their continuous administration is recommended only in the solution of conditions associated with conversion.
Calcium resonium - a non-absorbable resin, ion exchanger, after administration in the intestine releases calcium ions and binds potassium. Thus, the gradual removal of potassium in the stool takes place.
↑Jump up to:a b PARHAM, Walter A, Ali A MEHDIRAD and Kurt M BIERMANN, et al. Hyperkalemia revisited. Tex Heart Inst J [online] . 2006, vol 33, no. 1, pp. 40-7, also available from < https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1413606/?tool=pubmed >. ISSN 0730-2347.