Congenital Heart Defects

Congenital heart defects (CHDs) are among the most common congenital malformations. They affect about 1% of live births. The most common CHDs are ventricular septal defects (accounting for almost 42% of all CHDs), atrial septal defects (almost 9%) and aortic or pulmonary stenosis [1]. Sometimes malformations can appear in combination as complex heart defects.
In general, congenital malformations of the circulatory system account for more than 40% of all registered congenital malformations in the Czech Republic [2].
About half of all CHDs manifest as heart failure and/or cyanosis, and listening heart findings as early as the first week of life [3], most often (open ductus arteriosus (Botallo's duct), large vessel transposition, hypoplastic left heart, Fallot's tetralogy, and pulmonary atresia) [4]. Sometimes the symptomatology is non-specific, infants may experience increased sweating, drinking problems and indigestion, in adolescents reduced performance and shortness of breath [5].
Thanks to quality prenatal care, more than 40% of CHDs in the Czech Republic are diagnosed prenatally [6].
CHD Classification
Heart defects are traditionally divided into cyanotic and acyanotic, and further defects with left-to-right shunts, right-to-left shunts (the direction affects the pressure gradient and shunt location), and defects without a shunt.
| Congenital Heart Defects | ||
|---|---|---|
| Acyanotic | Cyanotic | |
| without shunts | left-to-right shunts | right-to-left shunts |
| aortal stenosis | ventricular septal defect | tetralogy of Fallot |
| pulmonary artery stenosis | atrial septal defect | transposition of the great vessels |
| coarctation of the aorta | an open ductus arteriosus | left heart hypoplasia |
| interruption of the aortic arch | defect of the atrioventricular septum | pulmonary atresia |
| heart position anomalies (ectopia cordis and dextrocardia) | partial anomalous return of pulmonary veins | tricuspid atresia |
| Lutembacher syndrome | complex single ventricle | |
- CHDs without a shunt
-
 Aortic Stenosis
Aortic Stenosis -
 Coarctation of the Aorta
Coarctation of the Aorta


- CHDs with a left-to-right shunt
-
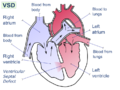 Ventricular Septal Defect
Ventricular Septal Defect -
 Atrial Septal Defect
Atrial Septal Defect -
 Patent ductus arteriosus
Patent ductus arteriosus -
 Atrioventricular Septal Defect
Atrioventricular Septal Defect




- CHDs with a right-to-left shunt
-
 The Tetralogy of Fallot
The Tetralogy of Fallot -
The Transposition of the Great Vessels
-
Hypoplastic Left Heart Syndrome
-
 Tricuspid Atresia
Tricuspid Atresia


Life-threatening CHDs
Critical VSVs endanger the patient's life due to heart failure and/or hypoxemia. They require urgent resolution.
Cyanotic defects have cyanosis (right-left shunt), intangible pulse, cold extremities, heart murmur, tachypnoea, dyspnoea, tachycardia and hepatomegaly.[7] Acyanotic defectsare accompanied by either murmurs or signs of congestive heart failure.[8]
Diagnosis is performed on the basis of clinical examination (saturation, oxygen test, tachypnea, dyspnoea, pulsation in HK and DK, heart rate, listening findings, evidence of hepatosplenomegaly), echocardiography, chest X-ray (heart size, character of the lung drawing), and ECG (sinus rhythm, positive wave P in the 1st lead and aVF, direction of the QRS axis to the right)[7].
- Uncorrected transposition of great vessels
- The aorta is connected to the front of the right ventricle and the pulmonary artery is connected to the back of the left ventricle. Systemic and pulmonary circulation work separately. It occurs in isolation or together with a ventricular septal defect, rarely with other defects. Cyanosis and tachypnea are clinically present due to hypoxemia.
- The Tetralogy of Fallot
- A complex of several defects – pulmonary stenosis, large ventricular septal defect (VSD), dextraposition of the aorta (misplaced aorta), and hypertrophy of the right ventricle. Due to a septal defect, the systolic pressure in both ventricles is balanced. Hypoxemia is exacerbated by the pulmonary stenosis (decreased lung flow). In infancy, it manifests as hypoxic attacks (a sudden worsening of cyanosis, tachypnoea, anxiety, and weakness).
- Hypoplastic Left Heart Syndrome
- The cavity of the left ventricle and the left atrium are small, stenosis or atresia of the mitral and aortic valves, hypoplasia of the ascending aorta. While aortic coarctation, frequent endocardial fibroelastosis, are present in 80% of cases. The right ventricle is hypertrophic and dilated – cardiac output is reliant on the activity of the right ventricle, the aorta is filled with a right-left shunt through a patent arterial ductus.
- It manifests as heart failure in the 2–4. day of life (at the closure of the ductus arteriosus), which leads to the development of shock and acidosis.
- Coarctation of the Aorta
- The narrowing of the aorta in the area of the aortic isthmus (rarely in the thoracic or abdominal aorta). It is often associated with other birth defects. The typical manifestation is weakened pulse on the femoral arteries (the difference in saturation between the upper and lower limbs). Then after ductal occlusion, left ventricular overload, decreased cardiac output, and the development of heart failure and shock occur. Sometimes the initial symptoms may be non-specific (poor food intake, failure to thrive, dyspnoea).
- Aortal and Pulmonary Stenosis
- The severity depends on the degree of stenosis. It manifests itself in heart failure, usually already prenatally.
- Pulmonary atresia with intact ventricular septum
- A rare but life-threatening defect. It often leads to the formation of aortopulmonary collateral. It is usually treated surgically immediately after birth, rarely and prenatally.
- Septal Defects
- The risk depends on the extent and location of the defect. They are usually associated with other birth defects. Extensive ventricular septal defects are the riskiest.
- Patent Ductus Arteriosus
- It connects the isthmus of the aorta and the lungs. It occurs physiologically in the fetus, after delivery it closes functionally within 10–18 hours and definitely within 3 weeks. Pathological persistence is most often present in preterm babies. It is clinically manifested by heart failure (due to increased lung flow) and the development of shock.
The Most Common CHDs in Adults
CHD in adults is often associated with the development of specific complications such as: infectious endocarditis, arrhythmias, hematological complications, Eisenmenger's syndrome and complications in pregnancy,
The Most Common CHDs:
- atrial and ventricular septal defects,
- coarctation of the aorta,
- the tetralogy of Fallot,
- aortal stenosis and aortal insufficiency
- bicuspid aortal valve,
- pulmonary stenosis,
- Ebstein anomaly,
- corrected transposition of large vessels,
- Lutembacher syndrome,
- Patent Botallo duct.
Links
Related articles
External Links
References
- ↑ JANOTA, Jan – STRAŇÁK, Zbyněk. Neonatologie. 1. edition. 2013. ISBN 978-80-204-2994-0.
- ↑ ŠÍPEK, Antonín – GREGOR, V. – ŠÍPEK, Antonín jr.. Incidence vrozených srdečních vad v České republice – aktuální data [online]. Ceska Gynekol, ©2010. [cit. 2022-02-02]. <https://www.ncbi.nlm.nih.gov/pubmed/20731304>.
- ↑ JANOTA, Jan – STRAŇÁK, Zbyněk. Neonatologie. 1. edition. Mladá fronta, 2013. ISBN 978-80-204-2994-0.
- ↑ GOMELLA, TL. Neonatology : Management, Procedures, On-Call Problems, Diseases, and Drugs. 6. edition. Lange, 2009. ISBN 978-0-07-154431-3.
- ↑ MUNTAU, Ania. Pediatrie. Grada edition. 2014. ISBN 9788024745886.
- ↑ JANOTA, Jan – STRAŇÁK, Zbyněk. Neonatologie. 1. edition. 2013. ISBN 978-80-204-2994-0.
- ↑ a b JANOTA, Jan – STRAŇÁK, Zbyněk. Neonatologie. 1. edition. Mladá fronta, 2013. ISBN 978-80-204-2994-0.
- ↑ GOMELLA, TL. Neonatology : Management, Procedures, On-Call Problems, Diseases, and Drugs. 6. edition. Lange, 2009. pp. 436-443. ISBN 978-0-07-154431-3.
Bibliography
- KLENER, Pavel. Vnitřní lékařství. 3. edition. Galén, 2006. pp. XV, 275. ISBN 80-7262-430-X.
- TASKER, Robert C. – MCCLURE, Robert J. – ACERINI, Carlo L.. Oxford Handbook of Paediatrics. 1. edition. Oxford University Press, 2008. pp. 242. ISBN 978-0-19-856573-4.
- OŠŤÁDAL, Bohuslav – VÍZEK, Martin. Patologická fyziologie srdce a cév. 1. edition. Karolinum, 2003. ISBN 80-246-0597X.
- ZEMAN, Miroslav – KRŠKA, Zdeněk. Speciální chirurgie. 3. edition. Galén, c2014. pp. 305-315. ISBN 9788074921285.

{kind=link}
{kind=link}