Basal cell carcinoma/PGS

Basal cell carcinoma is the most common human malignancy. It very rarely spreads metastatically, but it can grow infiltratively into surrounding tissues and destroy tissues locally. It usually occurs sporadically, but there is a syndrome of nevoid basal cell tumors, which is associated with the occurrence of basal cell carcinomas.
Epidemiology[edit | edit source]
Basal cell carcinoma is the most common malignant tumor, accounting for 70% of all cases of malignant skin tumors.
Risk factors[edit | edit source]
- Exposure to UV radiation.
- Exposure to arsenic.
- Exposure to coal tar.
- Skin phototype with fair skin, blue eyes and red hair.
- Immune system disorder.
- Terrain of some dermatoses (e.g. xeroderma pigmentosum).
Clinical picture[edit | edit source]
Basal cell carcinoma usually begins to appear in the fourth decade. If it appears at a younger age, it usually behaves more aggressively. It can appear anywhere on the skin, in places exposed to sunlight, less often in places protected from the sun.
The typical lesion is an ulcerated papule or nodule with pearly pink to fleshy margins through which telangiectasias shine through. Bleeding, scarring and crusting may also occur. An aggressively growing tumor often manifests itself as a more pronounced ulceration, with an extensive aggressive tumor it can lead to the destruction of organs such as the eye, ear or nose. The clinical picture can be quite variable, the lesion can resemble other skin pathologies, incl. malignant melanoma.
The lesion is usually not painful, pain is usually a sign of perineural spread. In the case of preauricular and facial localization, perineural spread can also cause a noticeable sensorimotor deficit.
Local recurrences are relatively common. Metastatic spread is rare, the overall risk of metastatic spread is estimated to be 0.1%. Risk factors for metastatic spread are mainly the size and depth of tumor invasion. With a tumor diameter above 5 cm, the risk of metastatic spread is estimated to be 20–25%, if the tumor is larger than 10 cm, the risk of metastatic spread is estimated to be 50%. The target of metastases are mainly local lymph nodes, lungs and bones. Tumors larger than 5 cm are associated with a significant risk of mortality and morbidity.
Patogenesis[edit | edit source]
It is assumed that basal cell carcinoma originates from stem cells located in the area of the hair follicle, especially in the area below the infundibulum (bulge). Basal cell tumors have a profile of expressed keratins similar to the deep parts of the hair follicle and thus differ from cells of the stratum basale of the epidermis.
Basal cell carcinoma cells usually express the following molecules:
- keratins 5, 6 a 14,
- integrins α2 a β1,
- CD10,
- p63,
- α6 integrin.
For a number of other markers, conflicting results or occasional positivity have been published.
- keratins 15 a 19,
- p63.
Normally, the CD34 molecule is not expressed. Let us note, however, that especially older works represent only relatively small sets.
A key role in the pathogenesis of basal cell carcinoma is played by signals, which involve the Sonic Hedgehog and the Wnt/β-catenin signaling cascade.
Basal cell carcinoma is also a tumor where the stroma plays a key role. Already in the early 1960s, it was demonstrated that if basal cell carcinoma cells are transferred without stroma, they degenerate and die, whereas if stroma is also transferred, the tumor continues to grow. Expression of a number of genes unusual for the stroma of normal fibroblasts in the dermis was demonstrated in the tumor stroma.
Histopatology[edit | edit source]
Histopathological diagnosis is an essential diagnostic modality that differentiates basal cell carcinoma from macroscopically similar lesions. Both tick biopsy and shave biopsy are not suitable, complete excision should be performed.
Traditionally, basal cell carcinomas are classified as undifferentiated (solid) and differentiated if the cells show signs of, for example, sebaceous, eccrine, or other differentiation. For the assessment of the behavior of the tumor, this division is less important, the assessment of the growth pattern is key.
Undifferentiated basal cell carcinomas[edit | edit source]
The group of undifferentiated (solid) basal cell carcinomas can be divided into two groups:
- indolent-growing basal cell carcinomas, which include the superficial and nodular variant of basal cell carcinoma;
- aggressively growing basal cell carcinomas, which include infiltrative, metatypic, and morpheaform variants of basal cell carcinoma.
Superficial basal cell carcinoma[edit | edit source]
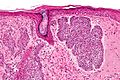
Atypical basaloid cells spreading parallel to the epidermis surface are typical for the superficial spreading variant of basal cell carcinoma. Despite the fact that the name might evoke spreading in the upper layers of the epidermis, tumor cells are found in the basal layers of the epidermis. The palisade-like arrangement of cells adjacent to the stroma and the slit-like spaces between these cells and the adjacent stroma are characteristic. Stromal cells can be found in these slits, which will be visualized when stained with alcian blue. Tumor cells can grow into hair follicles and eccrine glands. Mitoses are not numerous.
Melanin pigmentation may occur in the tumor cells and in the histiocytes in the adjacent stroma. Sometimes there is a rather pronounced striated lymphoid infiltrate.
Nodular basal cell carcinoma[edit | edit source]
The nodular variant of basal cell carcinoma is the most common variant of basal cell carcinoma. Histologically, the nodular variant is characterized by the presence of nests of basaloid cells in the papillary and reticular dermis, the size can vary from tiny to relatively large. Slit-like retractions are evident in the adjacent stroma. Differentiated cell elements can also be trapped in the tumor. Mitoses and necroses are uncommon. In approximately one third of cases, the coexistence of the nodular and superficial variants is evident, and the coexistence of the micronodular variant is also quite common.
There are myxoid changes in the adjacent stroma, fibroblasts are not abundant. Discrete islands of calcification may appear in the stroma. Abundant slit-like retractions can cause the tumor nest to move into the deeper layers of the dermis.
Melanin pigmentation may occur in tumor cells and in histiocytes in the adjacent stroma.
Micronodular basal cell carcinoma[edit | edit source]
The micronodular variant of basal cell carcinoma usually manifests macroscopically as a plaque-like, poorly demarcated induration. Tumor cells cluster into uniform nests similar to the nodular variant, only they are smaller and more irregularly scattered. They can reach the dermis or even the subcutaneous tissue. Recurrences are therefore more frequent after excisions. A stromal reaction is visible around the nests. Retraction slit-like spaces are not common.
Morpheaform basal cell carcinoma[edit | edit source]
The morpheaform (also sclerosing) variant of basal cell carcinoma represents an aggressively growing basal cell carcinoma. Macroscopically, it usually appears as a white to yellow sunken fibrotized scar that is usually not ulcerated and usually does not bleed.
The characteristic picture is slender columns of basaloid cells, usually one to two cells wide, sometimes more. These columns are embedded in the dens and low cellular fibrous stroma. Necrosis of individual cells may be present, mitoses also appear. Slit retractions are not common.
Infiltrating basal cell carcinoma[edit | edit source]
The infiltratively growing variant of basal cell carcinoma consists of irregular and variously sized nests to columns of cells. Mitoses and individual cell necrosis tend to be clearly visible. Sometimes slit-like retraction is captured. Tumors are poorly defined and therefore recurrences are frequent.
About a third of cases contain an admixture of the nodular variant of basal cell carcinoma.
Metatypical basal cell carcinoma[edit | edit source]
A metatypical variant of basal cell carcinoma, possibly also basosquamous carcinoma, is an aggressive growth form of basal cell carcinoma. Histologically, the tumor is made up of jagged streaks growing into the structures of the dermis. Abortive palisade is evident. Tumor cells have a basaloid morphology. Cytoplasmic bridges can be caught between tumor cells, intracytoplasmic keratinization can be seen. Admixture of the nodular or superficial variant is quite common.
Differentiated basal cell carcinomas[edit | edit source]
Differentiated basal cell carcinomas are characterized by the fact that basal cell carcinoma cells show a certain differentiation. This differentiation does not affect prognosis in any way.
Keratotic basal cell carcinoma[edit | edit source]
Keratotic basal cell carcinoma, also known as pilar basal cell carcinoma, appears histologically as large nests of basaloid cells surrounding central keratinization and degeneration. The central cyst is usually filled with keratin and parakeratotic detritus. Sometimes the cyst is filled with a layer of granular cells. Calcifications may also be present. The stroma is not prominent, mitotic activity is minimal and individual necrosis is at most rare. True hair formation does not occur in the lesion.
Infundibulocystic basal cell carcinoma[edit | edit source]
Infundibulocystic basalioma forms elongated round structures filled with keratinous masses, which are bordered by a stratifying epithelium with a distinct stratum granulosum and a distinct outer layer of basaloid cells.
In the differential diagnosis with trichoepithelioma and trichofolliculoma, the key is that the typical structures of follicular differentiation are missing and, on the contrary, there are often slit-like clefts between the stroma and the tumor itself.
Follicular basal cell carcinoma[edit | edit source]
Occasionally, basalioma differentiation may be similar to pilomatrixoma, where nests of proliferating basaloid cells are overlain by shadowy cells with eosinophilic cytoplasm and an indistinct nucleus (anuclear morphology). Calcifications may also be present. In the differential diagnosis, it is essential that follicular basal cell carcinoma is characterized by the absence of mitoses, apoptotic cells and high-grade nuclear atypia.
Pleomorphic basal cell carcinoma[edit | edit source]
Pleomorphic basal cell carcinoma is a variant of other types, especially nodular basal cell carcinoma. It is characterized by the fact that cells with huge homogeneous nuclei are scattered or even congested in the tumor. These cells are aneuploid but do not worsen the prognosis; apparently it is more a manifestation of senescence than a deterioration of biological behavior.
Basal cell carcinoma with sweat duct differentiation[edit | edit source]
A small number of especially nodular basal cell carcinomas may show signs of eccrine or, rarely, even apocrine differentiation. Tubules formed by eosinophilic cells are embedded in otherwise typical aggregates of basaloid tumor cells.
Basal cell carcinoma with sebaceous differentiation[edit | edit source]
A basal cell carcinoma with sebaceous differentiation can be distinguished from a sebaceous adenoma in particular by the fact that more than 50% of the cells on a section of the tumor are cells of the germinal layer. Slit-like retractions of the stroma are usually captured, the stroma does not react desmoplastically, the tumor is usually more regular and does not tend to spread pagetoidally.
Pinkus fibroepithelioma[edit | edit source]
Pinkus fibroepithelioma usually appears in the gluteal groove or lower trunk as a pink or fleshy red nodule with a retracted lower edge. Macroscopically, it may resemble seborrheic keratosis. Microscopically, the tumor consists of strips of basaloid epithelium embedded in a myxoid stroma or in a stroma with abundant spindle cells and significant collagen production, slit-like retractions are visible.
Gallery[edit | edit source]
- Macroscopic appearance of basal cell carcinoma

Basal cell carcinoma in the preauricular region.

Basal cell carcinoma on the bridge of the nose.

Basal cell carcinoma in the back area.

Pigmented basal cell carcinoma on the wing of the nose.




- Nodular variant of basal cell carcinoma

H&E

H&E
H&E

H&E




- Superficial variant of basal cell carcinoma

H&E, 20x

H&E, 4x


- Fibroepithelial growth pattern of basal cell carcinoma

H&E,
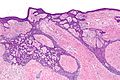
H&E,

H&E,

H&E,

H&E,





Links[edit | edit source]
Virtual preparations[edit | edit source]
https://www.pathowiki.org/pathowiki/index.php/Hauptseite
Related articles[edit | edit source]
Literature[edit | edit source]
- MILLS, S.E., et al. Sternberg's Diagnostic Surgical Pathology. 5. edition. Lippincott Williams & Wilkins, 2012. ISBN 9781451152890.
- CROWSON, A.N.. Basal cell carcinoma: biology, morphology and clinical implications. Mod Pathol [online]. 2006, vol. 19 Suppl 2, p. S127-47, Available from <http://www.nature.com/modpathol/journal/v19/n2s/full/3800512a.html>. ISSN 0893-3952.
- SELLHEYER, K.. Basal cell carcinoma: cell of origin, cancer stem cell hypothesis and stem cell markers. Br J Dermatol. 2011, vol. 164, no. 4, p. 696-711, ISSN 1365-2133.