Small intestine atresia and stenosis

Duodenal atresia and stenosis[edit | edit source]
The incidence of atresia and stenosis is 1:5000-10000. In 30 % of patients is co-occuring with Down syndrome and more than 50 % of patients have associated congenital disorders.
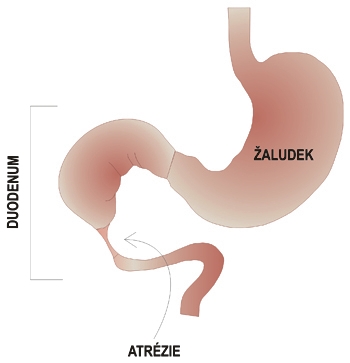 Duodenal atresia
Duodenal atresia

Clinal progression[edit | edit source]
There is polyhydramnios during the prenatal period, because of halted circulation of amniotic fluid. We can appreciate so called double bubbles sign - bubbles filed up with fluid. In the postnatal period, the complete obstruction is formed and within the first 24 hours the clinical sign of superior ileus develops which manifests by severe bilious vomiting. In 90 % the obstruction are found below the papilla of Vater. In remaining 10 % of cases, the vomit is non-bilious (do not contenct bile). The physician can see elevated epigastrium and depressed hypogastrium (boat-like abdomen), the peristalsis is visible. Failure to pass meconium is present. In partial obstruction, the clinical manifestation is delayed.
Diagnosis[edit | edit source]
The prenatal diagnosis is carried out by ultrasound screening. The postnatal diagnosis includes native X-ray of the abdomen which shows the typical two bubbles or levels, this counts for stomach and distended duodenum. In most of the cases the gas is absent in the distal part of GIT. We are able to suction more than 20 ml of fluid from a stomach by the nasogastric tub. The normal volume of fluid in the stomach is 5 ml. We proceed by insufflation the gas to the stomach which make possible to reproduce the image of two bubbles on X-ray. For definitive diagnosis and exclusion of possible malrotation or volvulus we perform a contrast X-ray the upper part of GIT.
Treatment[edit | edit source]
Treatment is surgical, the common procedure is duodeno-duodenal anastomosis.
Atresia and stenosis if the jejunum and ileum[edit | edit source]
The incidence of atresia and stenosis is 1:1500.
Clinal progression[edit | edit source]
There is a polyhydramnios in the prenatal period. The postnatal period is marked by the development of clinical presentation of middle ileus within the first 36 hours which cause bilious vomiting. The abdomen is distended, the breathing difficulties are present - dyspnea because of the the high position of the diaphragm. Failure to pass meconium is also present. A dehydration develops with hypochloremia and weight loss.
Diagnosis[edit | edit source]
The diagnosis is already visible by the ultrasound in the prenatal period - the dilation of the bowel. In the postnatal period we use native X-ray of the abdomen.
Treatment[edit | edit source]
Treatment is surgical, which consist of removing the part of gut with atresia or stenosis part and end-to-end anastomosis.
Links[edit | edit source]
Related articles[edit | edit source]
- Vrozené atrézie a stenózy gastrointestinálního traktu
- Syndrom arteriae mesentericae superioris
- Malrotace střeva a volvulus
- Mekóniový ileus
- Megacolon congenitum
Literature[edit | edit source]
ŠNAJDAUF, Jiří a Richard ŠKÁBA. Dětská chirurgie. 1. vydání. Praha : Galén, 2005. ISBN 807262329X.
HOLCOMB III, George W., J. Patrick MUPRHY a Daniel J. OSTLIE. Ashcraft's Pediatric Surgery. 6. vydání. Elsevier, 2014. ISBN 145574333X.
MUNTAU, Ania Carolina. Pediatrie. 4. vydání. Praha : Grada, 2009. s. 365. ISBN 978-80-247-2525-3.
Kategorie:Pediatrie Kategorie:Gastroenterologie Kategorie:Chirurgie