Choking

Shortness of breath is a subjective feeling of difficulty and labored breathing. Suffocation is a pathophysiological process resulting in impaired oxygen transport to target tissues, accompanied by objective clinical signs of respiratory distress [1]. The term dyspnoea describes objective signs of dyspnea, ie what can be observed in a mental patient (tachypnoea, orthopnoea).
Subjective manifestations of dyspnoea: Feeling of shortness of breath or lack of air. The patient is anxious.
Objective symptoms of suffocation: tachypnea, soft chest retraction, alaric deflection, open mouth breathing and gasping for breath, rattling breath, bubbling of retained secretion, wheezing and wheezing in the exhalation, cyanosis of the mucous membranes, silence above the chest even during hard breathing movements (complete obstruction) airways), orthopedic position. [2] [1]
Causes of dyspnea:
- external (preventing air from entering the lungs),
- internal (disorder of oxygen transfer to tissues).
Distribution of dyspnea according to manifestations:
- shortness of breath when inhaled (acute subglottic laryngitis, acute epiglottitis, pablan laryngotracheobronchitis, foreign body aspiration, allergic swelling of the larynx and subglottic space),
- shortness of breath on exhalation (acute bronchiolitis, bronchial asthma),
- shortness of breath during inhalation and exhalation (acute bronchopneumonia).
Distribution of dyspnea by course:
- acute (bronchial asthma, body aspiration, acute bronchiolitis, heart failure, pneumonia, pneumothorax, epiglottitis, laryngitis, chest trauma, neuromuscular diseases),
- chronic (incorrectly treated asthma, cystic fibrosis, bronchopulmonary dysplasia, congenital heart defects, extreme obesity, interstitial lung processes, repeated aspirations, neuromuscular diseases, chronic upper airway obstruction).
Shortness of breath can be a manifestation of:
- insufficient tissue oxygen supply;
- pathological irritation of the respiratory center in the elongated spinal cord;
- changes in the quality and quantity of respiratory effort.
Causes of shortness of breath
Respiratory dyspnoea
- Obstruction type;
- usually with stridor;
- is either inspiratory (laryngeal obstruction) or expiratory (bronchial), or combined;
- sleep apnea syndrome - breathing movements are preserved;
- in young children at the level of the nasopharynx in pharyngeal hypertrophy;
- in older children at the level of the mesopharynx with hypertrophy of the palate;
- in obese adults by tongue root entrapment.
- Newborns with choanal atresia - cyclic dyspnea with cyanosis;
- the newborn cannot normally breathe through his mouth (except for yawning and crying);
- it is due to the high larynx that allows it to otherwise suck, breathe and swallow at the same time…;
- but it doesn't work, CO2 accumulates in the body, irritating the center to yawn; the plot repeats itself.
- Special form of respiratory dyspnea - respiratory muscle paralysis, chest compression, emphysema, pulmonary atelectasis, pneumothorax, effusion…;
- the airways are free, so the stridor is missing.
Dyspnoea cardiac
- manifestations of tachypnoea, often seizures at night, pain in the heart landscape, stridor missing.
Dyspnoea due to hematological causes
- in anemia, oxygen-carrying block… .;
- pallor, stridor missing.
Dyspnoea from CNS disorders
- respiratory center depression - opiates, coma, coma, cerebral edema, spinal cord paralysis…;
- breathing is irregular, impaired consciousness, cyanosis, stridor is secondary to a sunken tongue.
Laryngeal dyspnea
From the ENT's point of view, shortness of breath during laryngeal obstruction occupies a special place, so let's set it aside here.
- It is inspirational, the stridor is present, the jugulum, the ankle holes and the intercostal space are drawn in;
- auxiliary respiratory muscles are involved;
- stridor - a mixture of tones and noises due to air swirls and oscillations in the area of stenosis;
- soft tissue retraction into the chest - given by the increase in vacuum at the time of inhalation;
- it is often accompanied by cough, hoarseness, dysphagia, fever, restlessness.
Three stages of laryngeal dyspnea
Compensation stage
- The symptoms described above are present;
- inspiration is prolonged at the expense of the break between expiration and inspiration;
- breath is regular, blood circulation is good;
- causal treatment is possible.
Decompensation stage
- Shallow tachypnoea, enhanced inspiratory stridor;
- often motor restlessness, crying in children;
- in connection with odynophagia (epiglottitis), apathy and analgesic behavior are common due to pain and exhaustion !!;
- children and adults occupy a sitting position, leaning forward with their mouths ajar and their chins outstretched;
- the lying infant tilts his head so that the entrance to the pharynx is as large as possible;
- circulatory and acral cyanosis begins;
- this stage is alarming, especially if it arose rapidly in the case of a child or a cardiopulmonary patient;
- treatment must immediately clear the airways;
Suffocation stage - asphyxia
- Irregular breathing, obesity and cyanosis;
- if suddenly → acidosis, heart failure, respiratory arrest occur;
- this stage requires urgent resuscitation.
Completely sudden laryngeal obstruction
- Reflective respiratory arrest - in connection with laryngospasm, the patient does not show signs of respiratory effort, cardiac arrest occurs rapidly;
- paradoxical movements of the chest - the breathing effort intensifies, the diaphragm by its contraction causes a chest invasion.
Therapy
Symptomatic treatment
- acute subglottic laryngitis - corticoids, cold air inhalation (vasoconstriction and decongestion of the swollen mucosa)
- allergic edema - adrenaline, methylprednisolone, calcium, antihistamines
- oxygen therapy
- ensuring access to the airways
Causal treatment
- removal of a foreign body from the airways - Heimlich maneuver, bronchoscopic examination
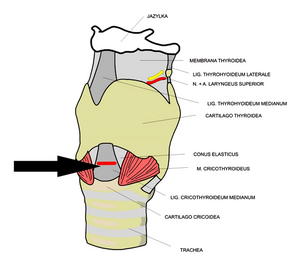
Localization of coniopuncture and coniotomy.

Urgent entry into the child's airways
Endotracheal intubation
- requires considerable experience, material equipment and pharmacological preparation of the patient.
Coniopuncture
Iron
- Impalment of the trachea in the area above the annular cartilage with injection needles or i.v. cannulas.
- The most suitable design is using a set on the Seldinger principle, ie a needle into the airways, through it a wire and then a dilator, at the end of which is a coniopuncture cannula.
- One of the cannulas may be insufflated into the airways by oxygen, the other must remain free to exhale.
Coniotomy
Iron
- Cutting of the trachea in the area above the annular cartilage, below the thyroid cartilage, where we intersect the cricothyroid ligament (lig. Conicum).
- Unsuitable for the risk of excessive devastation of the thin child's trachea and the risk of blood aspiration, especially from a severed thyroid gland.
Tracheostomy
Iron
- Surgical performance that requires experience, equipment and anesthesia.
Links
related articles
- Shortness of breath • Inspirational shortness of breath • Expiratory shortness of breath
- Respiratory insufficiency
Source
- BENEŠ, Jiří. Studijní materiály [online]. ©2007. [cit. 2009]. <http://jirben2.chytrak.cz/materialy/orl_jb.doc>.
Reference
- MIXA, V. Urgent skills in pediatrics. Pediatrics for practice [online]. 2007, vol. 8, vol. 5, pp. 307-310, also available from <http://www.pediatriepropraxi.cz/pdfs/ped/2007/05/12.pdf>.
- LEBL, Jan, Kamil PROVAZNÍK and Ludmila HEJCMANOVÁ, et al. Preclinical pediatrics. 2nd edition. Prague: Galén, 2007. pp. 106–107.
Kategorie:Otorhinolaryngologie Kategorie:Slovník fyziologie Kategorie:Kardiologie Kategorie:Pneumologie Kategorie:Vnitřní lékařství Kategorie:Neodkladná medicína Kategorie:První pomoc

{kind=link}